The pathology, the functional anatomy of clubfoot and the structural changes in its ligaments, tendon, and muscles, must be well understood to arrive at a smart approach to early non-surgical treatment this of deformity.
THE BASE OF UNDERSTANDING
To fully understand the pathology of the clubfoot, it is necessary to understand the ANATOMY of the healthy foot with no abnormalities. It is the base. The structure of the ACHILLES TENDON is the second element, knowledge of which cannot be overlooked. As the clubfoot is a three-dimension deformity, the specific “directions” of this pathology, closely related to the FOOT MOVEMENTS of the foot, must also be systematized.
HISTORICAL DISCUSSION
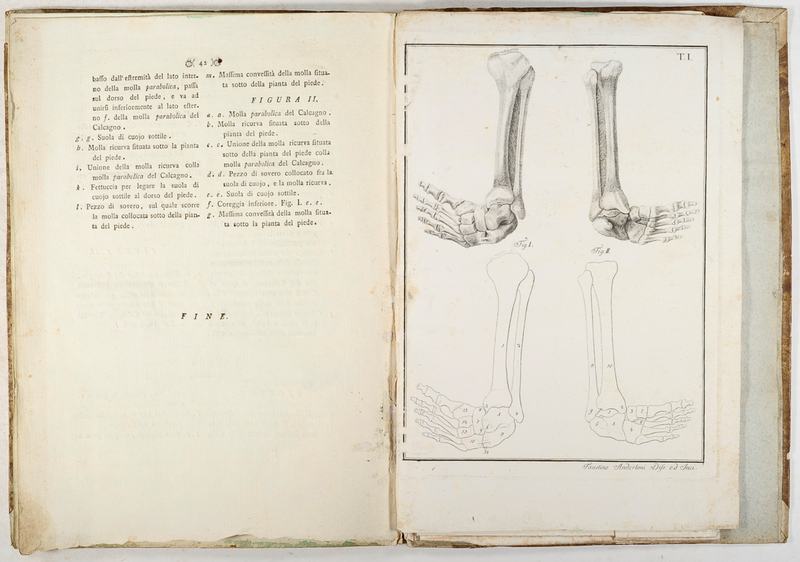
Pathology of the congenital clubfoot was well described already in 1803 by the Italian anatomist and professor Antonio Scarpa in (his) work “Memoria chirurgica sui piedi torti congeniti“. Scarpa noticed that the navicular bone, cubioid bone and calcaneus bone are medially shifted and inverted relative to the talus bone. At the same time, he believed that these muscles’, tendons’ and ligaments’ anomalies of the foot and leg were a secondary deformity of bone deformities. Many of the authors and researches have been keenly interested in pathology that forms the clubfoot. It was not an ignored topic but vividly discussed one. However, it was Dr. Ponseti, together with Dr. Ernesto Ippolito from Italy, who, since 1947, studied in-depth, from the histological point of view, many pathological and healthy feet from aborted fetuses (abortion between 16th and 24th week of pregnancy), stillborn babies and those who died shortly after labour.
“SOFT” PROBLEM
In congenital clubfoot selected bones are displaced relative to each other but the rotation of the bones (calcaneus, cuboid, navicular and cuneiforms) around the talus bone is the result not a cause of this deformity. This is the key to understand the problem of the deformity itself and its nonsurgical way of treatment, which is very innovative and, at the same time, relatively uncomplicated. The displacement of the individual bones relative to each other is caused by the very strong pulling of ligaments, tendons, and muscles. The problem is not the structure of the bones and their arrangement, although that is what it manifests itself. The problem is in the soft tissues. They have some anomalies that cause the movement of the tarsal bones and the change of their shape – a slight change, but still.

IMBALANCE
Lack of balance that occurs in the soft tissues: ligaments, tendons, joint capsules, muscles is one of the most important aspects of the clubfoot, influencing bone shifts inside the foot and deformities characteristic for the defect which become permanent during fetal life. The strength of the soft tissues forces the bones to be positioned specifically relative to each other, and this causes the bones, retained in this position, to deform slightly. Shortened sections of the soft tissues cause the rotation of the tarsal bones around the talus bone. Soft structures in the medial part of the foot become shorter, those in the lateral part – become stretched. Due to these unequal forces of the ligaments, tendons, and muscles acting on the foot, it becomes inverted, which causes the calcaneus bone to become varus. By shortening the plantar and medial parts of the muscles, the abduction of the forefoot (MTA – Metatarsus Abductus) takes place – the calcaneus bone locks under the talus bone and the remaining bones slide relative to each other. Too short Achilles tendon positions the foot in plantar flexion.
In that way, a three-dimensional deformity develops, because changing the position of one of the tarsal bones affects the position of the next.
The clubfoot is characterized by muscular atrophy and fibrosis of individual muscles and tendons.
ATROPHY
FIBROSIS
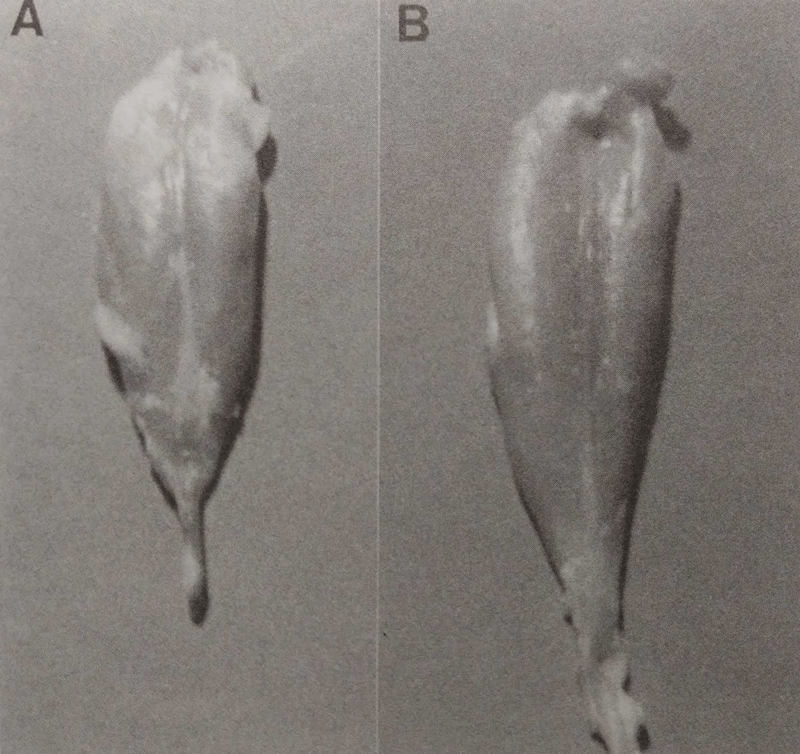
Muscle atrophy in clubfoot affects especially the posterior and medial muscles of the calf. The calf triceps and the posterior tibial muscles are fibrotic, have a smaller volume, are shorter, and smaller. In the photo beside, there is presented the calf triceps muscle: A. in the calf of a child with clubfoot, and B. in a normal, healthy calf. Some tendons and muscles or ligaments are slightly moved towards the medial side, e.g. the posterior tibial muscle, the extensor digitorum longus muscle or the extensor hallucis longus.


DEFICIENCY
At children with this defect, there is also a specific dominance of type I muscle fibres – they are slow-twitch fibres, which are assumed to be more durable, but also weaker. That means that they can work for a long time but their power is low. Children are born with a type II muscle fibres deficit and this deficit remains constant during development and is independent of age. Over 80% of children with congenital clubfoot have a poorly developed anterior tibial artery but even under these circumstances, the entire cardiovascular system develops properly. Veins and arteries, as well as numerous capillaries, supply the fibrotic muscles with oxygen, which allows them to work and keep the lower limb in good condition for many years.
CURIOSITY

BONE DISPLACEMENTS
From the uneven work of muscles and other soft structures, numerous changes occur in the position of the bones. Often these bones, very soft and susceptible to deformities, due to shifts relative to each other, slightly change their shape or are slightly smaller than in a normal, healthy foot.
By following the shifted bones, you can see that:
The calcaneus bone (green) is blocked under the talus. A shortened Achilles tendon pulls the back of the locked bone upwards causing the equinus position of the heel. This makes the calcaneus very difficult to feel under the fat pad. This position of the calcaneus gives a strong plantar flexion in the ankle mortice. The inclination of the calcaneus bone around the talus bone (red) gives the heel a varus alignment with the vertical axis of the talus and its blocade under the talus causes it to be adducted.
The talus (red) is also in the plantar flexion. In addition it is turned towards the middle and its side part is not covered with the navicular bone – you can feel the head of the talus bone and its exposed edge on the lateral side of the foot. The talus is smaller than in a healthy foot and its head is wedge-shaped. Sometimes the entire talus bone is a little flattened. Just below the head of the talus bone is the calcaneus – you can often mistake one for the other. A child’s head of the talus is only 0,5 cm in size.
Foot adduction is caused by the shifting of the navicular (yellow) to the medial surface of the talus head. The navicular then forms a joint only with the medial part of the head of talus so that the navicular often touches the medial malleolus. It happens that the bone is a little flattened and is wedge-shaped from the lateral side. The cuboid (orange) moves medially relative to the anterior tuberosity of the calcaneus and lowers. The 3 cuneiforms (blue) move downwards, positioning medially to the navicular. The metatarsal bones are in plantar flexion and adducted, which looks as if the foot was ‘broken’ halfway through.


SOURCES
RESEARCH & STUDIES:
1. Ponseti I.V.: “Congenital Clubfoot. Fundamentals of treatment.” (2nd edition)
2. Ponseti I.V., Campos J.: “Observations on Pathogenesis and Treatment of Congenital Clubfoot.”
3. Gradek J., Szafrański T., Michalak J.: “Leczenie wrodzonej stopy końsko-szpotawej metodą Ponsetiego z wczesnym zastosowaniem opatrunków gipsowych – doświadczenia własne.”
4. Windisch et al.: “A model for clubfoot based on micro‐CT data.”
5. Windisch G. et al.: “Anatomical study for an update comprehension of clubfoot. Part I: Bones and joints.”
6. Ippolito E. et al.: “Leg muscle atrophy in idiopathic congenital clubfoot: is it primitive or acquired?”
7. Gosztonyi G., Dorfmüller-Küchlin S. et al.: “Morphometric study of muscle in congenital idiopathic club foot.”
8. Isaacs H. et al.: “The muscles in clubfoot – a histological, histochemical and electron microscopic study.”
9. Gray D.H. et al.: “A histochemical study of muscle in clubfoot.”
10. Bohner-Beke A. et al.: “Lower leg atrophy in congenital talipes equinovarus.”
11. Fulton Z. et al.: “Calf circumference discrepancies in patients with unilateral clubfoot: Ponseti versus surgical release.”
12. Kerling A., Mellerowicz H. et al.: “The congenital clubfoot – immunohistological analysis of the extracellular matrix.”
13. Laurent R.: “Interet de la kinesitherapie complementaire au sein de la methode de Ponseti dans le traitement du pied bot varus equin congenital.”
PHOTOS & GRAPHICS:
1. A. Scarpa: “Memoria chirurgia sui piedi torti congenita”
2. Tendons: Ponseti I.V.: “Congenital Clubfoot. Fundamentals of treatment.” (2nd edition)
3. Muscles comparison: Ponseti I.V.: “Congenital Clubfoot. Fundamentals of treatment.” (2nd edition)
4. Windisch G. et al.: “A model for clubfoot based on micro‐CT data.”
5. Other: own