SOMETHING EXTRA…
Generally, clubfoot, as it has already been explained in the article WHAT IS IT, have their own specific features that attribute them to this type of deformity of the lower limb, and not to another. However, some feet in their structure have or acquire additional features over those that are assumed to be assigned to clubfoot.
Atypical and complex feet are a type of feet that have additional characteristics created over time and by specific factors. Understanding the formation and structure of atypical and complex feet is quite significant because these feet require some changes in the method of their treatment, from plastering to the use of a derotation bar. Such feet may also react differently in the future, which can result in the relapse or the need for possible surgical treatment.

ATYPICAL CLUBFOOT
The atypical clubfoot is one of the types of a non-typical foot deformity. Importantly, it is the type of only and exclusively idiopathic deformity. This means that the child has no other syndromic, neurological or teratogenic problems that could result in clubfoot deformity, including this particular foot anomaly. It is also difficult to unequivocally determine whether the foot will be “standard” or atypical purely on the basis of ultrasound examination. Despite the increasing diagnostic possibilities, its precise classification is still not possible. The atypical foot can be diagnosed with certainity immediately after birth and before any treatment. In addition to the standard features of clubfoot, atypical foot has additional features that are immediately apparent. However, a lot of experience is required from the doctor to be able to define them well. Ability to recognize the features of atypical foot sufficiently early is still a huge problem, hence it is likely to lead to the incorrect choice of the treatment method. This may be associated with potentiating its features, thus increasing the risk of turning into a complex foot. Atypical clubfoot is rather a rare condition – it affects less than 5% of children, which is a small percentage among other types of feet.
CHARACTERISTICS


The atypical foot does not show much adduction. It is rather moderate, which gives the illusion that treatment will be easier. Nothing could be further from the truth! The shortened plantar fascia causes all of the metatarsal bones to be plantar flexed, most notably the first one. A transverse crease is formed on the sole of the foot, running from the medial to the lateral of the foot.

The metatarsal bones are plantar flexed because the plantar fascia is shortened. This creates a deep transverse crease on the sole of the foot. Cavus is affected not only by the medial side of the foot, but also the lateral one. It looks as if the foot was broken in half at the midfoot.

The combination of the metatarsal plantar flexion and the strong pull of the heel through the short and thick Achilles tendon creates a deep crease above the heel. In spite of this, the foot is not stiff at the ankle joint. The outline and shape of the heel does not change. Seen from the sole, the heel is most often V-shaped or very tight U-shaped, whilst looking from the back, it seems very soft. Thick fat inside the heel makes the calcaneus difficult to feel, hence the impression that the heel is soft and hollow.

The plantar flexion of the first metatarsal bone caused by a too short plantar fascia usually makes the big toe point downwards (hyperextension). The remaining toes may be turned slighlty inwards or may also be hammer-shaped
``ATYPICAL``
In the atypical foot, the plantar fascia is short, which triggers a number of complications. The foot is even shorter than the ‘standard’ clubfoot. It is also a bit wider in the forefoot, but at the same time it is not chunky, its back does not contain as much fat as for example a complex foot. The atypical foot is not “chubby”. The plantar fascia, which attaches to the calcaneal tuberosity (underside of the calcaneus) on one side and attaches to the heads of the metatarsal bones on the other, causes all of these bones to be plantar flexed (downward), predominantly the first one. There is a crease on the sole of the foot, running from the medial to the lateral side of the foot. At the same time, the first toe is in a slight inferior hyperextension. Equinus is a combination of plantar flexion (by a shortened aponeurosis) of the forefoot and plantar flexion at the ankle joint, which is not very stiff by itself, but the short and thick Achilles tendon definitely restricts movement in that area. A deep crease forms above the heel.
COMPLEX CLUBFOOT
Complex clubfoot is a type of a non-standard type of deformity that occurs relatively often as compared to atypical clubfoot. What is important is that any type of foot can form into a complex foot. It does not matter whether the feet are idiopathic, syndromic, neurological or teratogenic, as complex foot depends on external factors such as poor plaster casting technique, frequently slipping down the casts or casting a swollen leg. Since this foot is the result of incorrect treatment, it is not diagnosed by ultrasound. Due to incorrectness, apart from the typical features of the clubfoot, the foot acquires specific additional attributes. It is also often described by doctors as “persistent” or “stubborn” clubfoot because after applying 4 or 5 plaster casts, the foot is still not corrected. Such foot is difficult to correct: stiff and tenacious. Typically, children who have this type of foot deal with major skin problems under the plaster cast: redness, wounds under the cast, abrasions, large swellings, bruises, which increases the complexity of the deformation (it is difficult to put on a plaster cast correctly, plaster cast slips off, the skin is stiff as with lymphoedema, the falling plaster cast creates new deformations or increases the already created ones, etc.). The risk of soft tissue surgery that may be necessary ranges from 3 to 5%.
CHARACTERISTICS

Since the plantar fascia is very shortened, the metatarsal bones are in the plantar flexion. As a result, the foot is very short (e.g. in the case of a unilateral defect, the foot with the defect may be shorter than a healthy foot by up to 1.5 cm), wide in the toes, has a high arch and a lot of fat on the top of the foot, which gives the impression as if the foot was swollen. Due to incorrectly applied plaster casts, the foot becomes stiff. The fat tissue is quite compact – it makes it difficult to perform foot compression before putting on the plaster cast (it is difficult to grab the foot properly because it is stocky).
Due to the too tight and often sliding plaster casts, the calcaneus is artificially pushed up, compressing the Achilles tendon so that it shortens even more, although it was not like that in the first place. It pulls the calcaneus strongly upwards, the external symptom of which is a deep crease above the heel. The outline of the heel and its shape are also changed: it is often misshapen, flattened, squashed or skewed. Thick fat inside the heel makes the calcaneus not easy to feel, hence the impression that the heel is soft and empty.
Since all the metatarsal bones are plantar flexed, an overly shortened plantar fascia forms a deep transverse crease on the bottom of the foot that is visible not only from the medial side of the foot (viewed from the side) but also from the lateral side. The heel is very swollen and quite soft to touch as if it was empty inside.
An excessively shortened plantar fascia causes the big toe to protrude. That is, it is hyperextended. The strength of the hyperextension depends on the degree of shortening of the plantar fascia: if the plantar fascia is very shortened, the big toe hyperextension is very large. The big toe also very often looks “pressed” into the foot, because the first metatarsal bone is shortened and plantar flexed due to an overstretched plantar fascia. This phenomenon is related to the so-called “windlass mechanism” described below.
WIDNDLASS MECHANISM
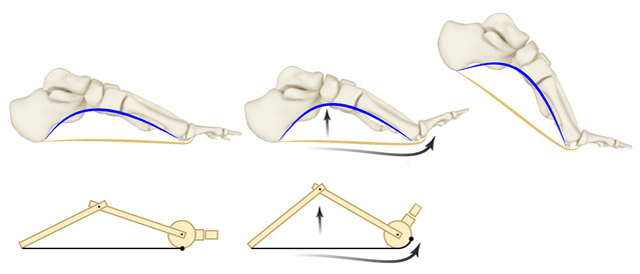
When the plantar fascia is shortened, the big toe automatically positions itself in the hyperextension as the longitudinal arch of the foot is lifted unnaturally, drawing the metatarsal bones to the calcaneus. The high longitudinal arch pulls the big toe extensors, and these, in turn, pull it upwards.
















TREATMENT MODIFICATIONS
Ponseti treatment is very effective and ensures that the feet are fully functional and are of normal appearance. This high effectiveness and ease of treatment affects many feet. However, sometimes there are cases where the feet do not respond to the standard treatment with this method so easily. These may include atypical and complex feet. The correctness of the treatment of atypical feet depends on the knowledge and experience of the doctor, who will come into contact with them. Therefore, it is important to choose it very consciously. Similarly, in the case of the treatment of complex feet – the doctor’s experience takes the lead here and it cannot be anyone “random”, as the treatment requires some modifications to the standard Ponseti method. Don’t worry though! These modifications are safe – they effectively correct deformation without the need for extensive surgical correction or they radically reduce the need for correction surgery. As early as 1994, Dr Vincent J. Turco advised against any surgical intervention on such feet, explaining that it was becoming even more grotesque. He was also the first to classify them as „atypical clubfoot”. In 2006, Dr Ignacio Ponseti together with his work colleagues informed about changes in the standard treatment protocol in order to be able to treat this type of feet as well. TREATMENT OF ATYPICAL AND COMPLEX FEET by the Ponseti method does not only involves modifications related to redressing or casting, but also the use of a different type of FOOT ABUDCTION BRACE (suggested Mitchell boots and brace) and its ADJUSTING other than “standard”. All of this is quite important and will affect the health of such feet in the future.
THE RISK OF RELAPSE
THE RELAPSE is one aspect that worries parents perpetually, regardless of whether a child has “standard” feet or atypical feet. For atypical and complex feet, the relapse rate is as high as 68%. This is quite a lot and one has to be prepared for all kinds of events. Unfortunately, so far no studies differentiate the risk of relapse separately for atypical feet and complex ones. If a relapse does occur, it is a standard procedure to return to casts as stated in the article on RELAPSES.
SOURCES
RESEARCHES & STUDIES:
1. Ponseti I.V.: “Congenital Clubfoot. Fundamentals of treatment.” (2nd edition)
2. Bolgla L.A., Malone T.R.: “Plantar Fasciitis and the Windlass Mechanism: A Biomechanical Link to Clinical Practice.”
3. Gupta A., Hakak A. et al.: “Atypical clubfoot: Early Identification and treatment by modification of standard Ponseti technique.”
PHOTOS & GRAPHICS:
1. Windlass mechanism
2. Other: own and thanks to people of good will