When to start the treatment of clubfoot?
4 April 2020
Incorrect casts
5 January 2023
The Ponseti method is not just a plaster cast „somehow” put on. This is a cast very PRECISELY put on. To be a correct one, the plaster cast needs to meet several really important requirements. What is a correct plaster cast in the Ponseti method?
PROGRESS
Above all and what should be emphasised at the very beginning: the plaster cast is applied by a doctor trained in the PONSETI METHOD together with a well-prepared plaster cast technician. The plaster cast must not be put on by a random employee of the hospital/clinic/cast room, without the presence of a doctor. Such a treatment is pointless.
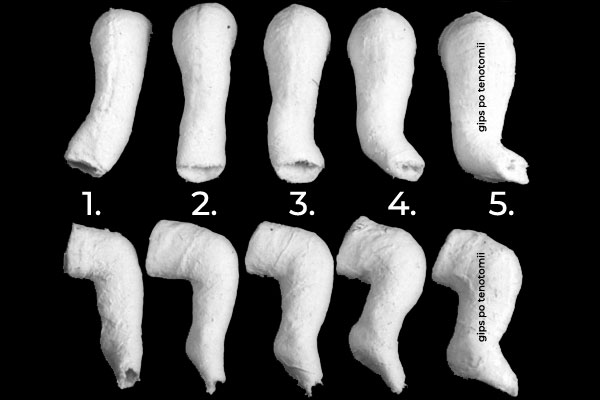
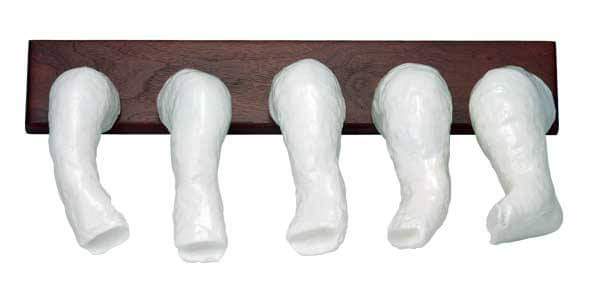
It should also be clearly stated that each plaster cast brings a change in the positioning of the foot. It means that each subsequent plaster cast sets the foot in a different position, closer to its natural, “healthy” shape. It can easily be observed, for example, in the picture below, showing the desired positions of each subsequent plaster cast. If it is not so – then the treatment is incorrect.
Of course, in majority of cases reported to us, the lack of progress in the shape of the plaster cast is explained with:
It is the foot’s fault. The foot is hard, difficult, resistant to treatment. It cannot be done.
Unfortunately, each statement like this makes us doubt if the person speaking really has the proper knowledge and experience in treating this defect with the Ponseti method. Each time when we hear explanations like the one above, we use the following counterargument (it really captivates us):
It is not the fault of the foot that it is what it is. It is the fault of improper plaster casting technique. If you claim the foot to be hard, resistant, tough, then take a look at your plaster casting technique. Most probably it is not proper nor sufficient, and you need to verify and improve it.
Dr. Jose Morcuende | Ponseti International Association

DETAILS
Putting on a plaster cast in the PONSETI METHOD is not a crude, primitive procedure, as it is seen by many doctors (and parents), saying: “What is it to put a plaster cast on? Nothing difficult.” Well, it turns out not to be as trivial as it seems. The plaster cast applied in the Ponseti method must meet certain conditions, and the details really matter – often they define the quality of the treatment
- FROM TOE TO GROIN – the Ponseti method plaster cast is a so-called long leg cast. It covers the whole leg: from the toes up to the groin.
- KNEE FLEXED AT 90° – in a correctly applied plaster cast, the knee is bent at 90° (or 110°-120° for ATYPICAL OR COMPLEX CLUBFOOT).

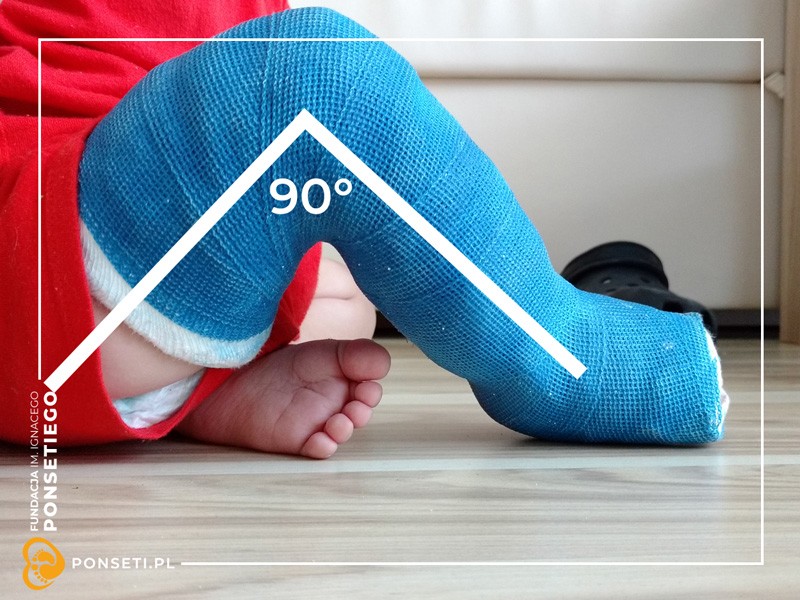
Such a plaster cast (long cast + bent knee) allows to immobilize the foot in the right position: this prevents the talus from rotating back into its original, improper position. Also, the soft structures (ligaments, tendons, tissues) are maximally, equally and slowly stretched. During such correction, joint surfaces change shape, matching the new, proper position. Soon we will describe it in more detail in a separate post.
- WELL MODELLED AND WELL SHAPED
A correct plaster cast is precisely modelled in the area of the ankle, heel and the whole foot. It can be said that the plaster cast has the shape of a foot. A child’s foot is wide near the toes and narrow near the heel; and so is the plaster cast. The heel in the plaster cast has the shape of a heel – it is not flattened. Near the groin the cast is slightly wider – to prevent it from squeezing the thigh, pressing or wounding it. The knee should also be moulded well, especially that there is a little more plaster there.




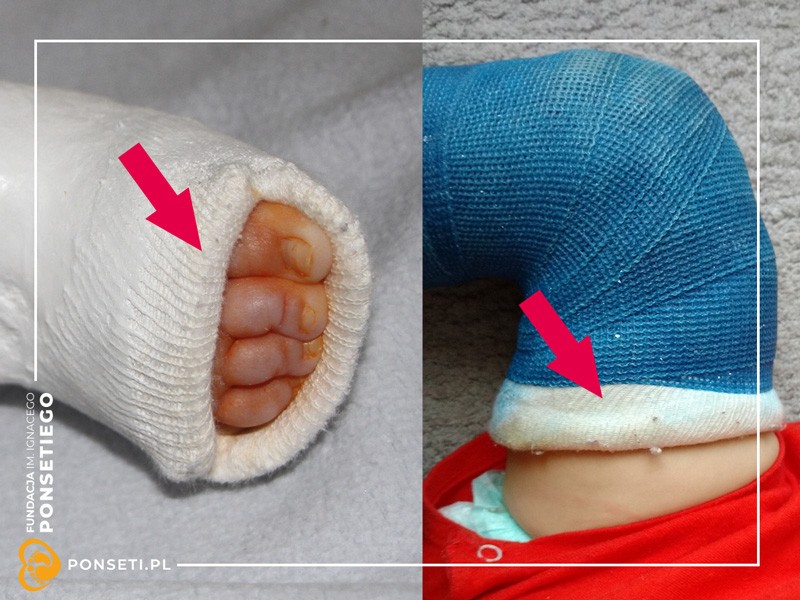
- VISIBLE TOES
The plaster cast should provide enough space for the toes – they should all be clearly visible, evenly distributed (in a line) and not squeezed. Also, the toes must not reach outside the cast. Later, this causes numerous complications (for example, contractures), which could have been avoided.






- RELATIVELY THIN
The plaster cast should be relatively thin not to burden the child with extra weight. At the same time, it should be strong enough to keep the foot in the right position and to stabilize the leg in the plaster cast so that it does not move, for example, at the knee. A thick, heavy, coarse and clumsy plaster cast indicates the not-well-developed technique of the person who applied it. Such a plaster cast may suggest that the person is not really familiar with casting according to the Ponseti method.
- NOT TOO TIGHT, NOT TOO LOOSE
Imagine that a leg is like a balloon filled with water and placed inside a pipe. When the plaster cast is too tight, the leg inside is swelling; veins, arteries, muscles are pressed. The toes are swelling as well. Such a plaster cast must be removed. Immediately! When the plaster cast is too loose, it cannot keep the foot in the right position, which has effect on the correction – that is, no correction. Such plaster casts often fall, and this… is not good. A plaster cast that is sliding or falling from the leg causes the foot to become COMPLEX. A plaster cast sliding down the leg must be removed IMMEDIATELY!
NICE TOUCH
It is good to secure the edges of the plaster cast (by the toes and by the groin) – then they do not hurt the skin. It is a good idea if the doctor puts a cotton tunnel on the leg, then applies the cast, and finally rolls the ends of the tunnel up onto the plaster cast. Secured like this, the edges of the plaster cast do not irritate the skin when the child is, for example, moving their legs. Also, such a tunnel prevents the plaster cast from crumbling or cracking at the edges.
Sometimes the standard white plaster cast is covered with synthetic cast (Soft Cast or Scotch Cast) to prevent it from crumbling, cracking or wearing off. This method is used with more active children who already crawl, try to stand or walk.

From time to time we will be writing about how a plaster cast should (or should not) look like, and why. Pay attention if your child’s plaster casts are not similar to the ones in the photos above. It is very important. A plaster cast may repair the foot, but it may also cause further deformities – for example, bend the tibia or fibula; cause the already mentioned complex clubfoot or overcorrected foot; deform the bones in the foot or ankle; to shift back the tibia and many more. Unfortunately, we observe all of these errors every day. We often see the long-term results of incorrect treatment – they may be hard to repair and may affect the functioning of the whole body. Be aware and if your doctor puts the plaster casts wrong – tell him/her about it and find a doctor who knows the Ponseti method.

{kind=link}
{kind=link}